
INCIDENCE
What is the incidence of CPP?
CPP, a gonadotropin-dependent precocious puberty, is a rare condition.2,3
What are the causes of CPP?
- CPP is caused by early activation of the HPG axis4
- CPP is most often idiopathic in girls, while boys are more likely to have organic causes4
What are the potential health implications of CPP?
Children with CPP may experience5-8:
- Expression of secondary sexual characteristics that are inconsistent with their age group
- Rapid bone maturation that results in shorter predicted adult height
DIAGNOSIS
How is CPP diagnosed?
If signs of early puberty are seen by the patient's family or family physician, a complete physical examination should be performed, including:
A focused medical history, including9:
- The precise rate and timing of growth
- A history of secondary sexual characteristic development
- Behavioral changes related to puberty
- A family history
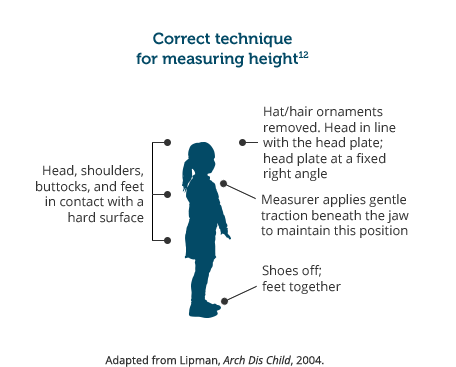
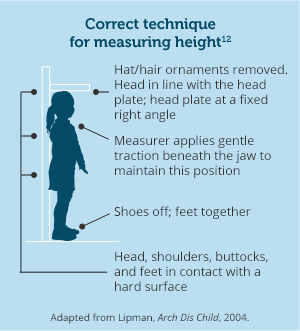
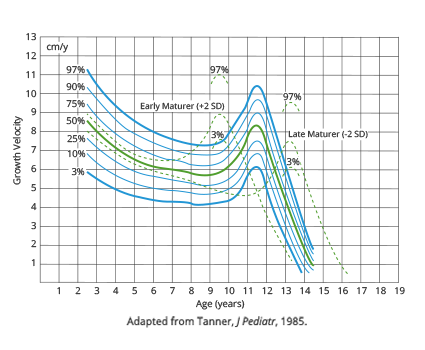
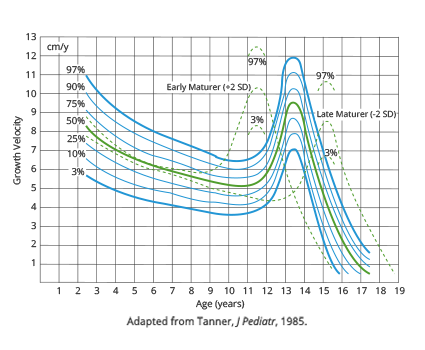
An accurate plotting of growth and evaluation of growth velocity10-12
Growth velocity chart10,11

A physical examination
Staging by using Tanner-Marshall protocol to evaluate pubertal development
Tanner-Marshall stage ≥2 before age of 8 in girls1
- Evaluation of breast development: Palpitation helps differentiate breast tissue from adipose tissue13
Tanner-Marshall stage ≥2 before age of 9 in boys1
- Evaluation of testicular development: A phallus length of 2.5 cm or more in flaccid state, or testicular volume of 4 mL or more is suggestive1
Girls6,14
Breast development
Stage 1 (Prepubertal)
No breast development,
only the nipple is raised.
Pubic hair growth
Stage 1 (Prepubertal)
No pubic hair. The vellus (fine hair) is not further developed than that on the abdomen.
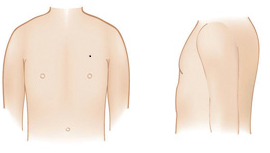
Boys7,14
Genital development

Stage 1 (Prepubertal)
The testes, scrotum, and penis are all about the same size and proportion as in early childhood.
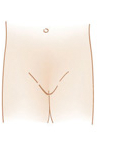
Pubic hair growth

Stage 1 (Prepubertal)
No pubic hair. The vellus (fine hair) is not further developed than that on the abdomen.
Adolescent Medicine Secrets. Philadelphia, PA: Hanley & Belfus; 2002:21-28.
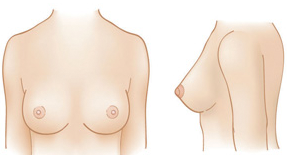
Girls6,14
Breast development
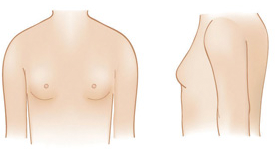
Stage 2
Breast bud stage. There is elevation of the breast and nipple as a small mound and enlargement of the areola diameter.
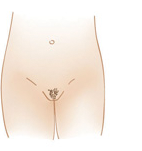
Pubic hair growth

Stage 2
Sparse growth of long, slightly pigmented, downy hair, straight or only slightly curled, appearing mostly along the labia.
Boys7,14
Genital development

Stage 2
The scrotum and testes have grown. There is a change in texture and some reddening of the scrotal skin.
Pubic hair growth

Stage 2
Sparse growth of long, slightly pigmented, downy hair, straight or only slightly curled, appearing mostly at the base of the penis.
Adapted from Brown RT. Adolescent growth and development. In: Holland-Hall C, Brown RT, eds.
Adolescent Medicine Secrets. Philadelphia, PA: Hanley & Belfus; 2002:21-28.
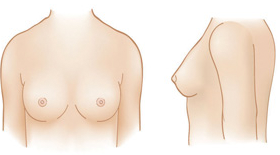
Girls6,14
Breast development

Stage 3
Further enlargement of the breast and areola with no separation of their contour.
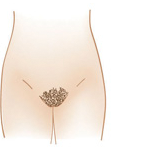
Pubic hair growth
Stage 3
Considerably darker, coarser, and more curled hair that is beginning to spread across the pubic area.
Boys7,14
Genital development

Stage 3
The penis has grown mainly in length (occurs first), followed by some increase in width. There is also growth of the testes and scrotum.
Pubic hair growth

Stage 3
Considerably darker, coarser, and more curled hair that is beginning to spread across the pubic area.
Adapted from Brown RT. Adolescent growth and development. In: Holland-Hall C, Brown RT, eds.
Adolescent Medicine Secrets. Philadelphia, PA: Hanley & Belfus; 2002:21-28.
Girls6,14
Breast development
Stage 4
The nipple and areola project to form a second mound above the level of the breast.
Pubic hair growth
Stage 4
The hair is now more like adult pubic hair, but the area it covers is smaller compared to most adults.
Boys7,14
Genital development

Stage 4
The penis is further enlarged in length and width with development of the glans (wider area at end of penis). The testes and scrotum have continued to grow, and there is further darkening of the scrotal skin.
Pubic hair growth

Stage 4
The hair is now more like adult pubic hair, but the area it covers is smaller compared to most adults. Hair has not yet spread to the inner thigh area.
Adolescent Medicine Secrets. Philadelphia, PA: Hanley & Belfus; 2002:21-28.
Girls6,14
Breast development
Stage 5
Projection of the nipple only. The areola now shares the general contour of the breast. There is no longer a second mound as in stage 4.
Pubic hair growth

Stage 5
The hair is now like adult pubic hair in both type and quantity. It is distributed in the classic triangle pattern and has spread to the inner thigh area.
Boys7,14
Genital development

Stage 5
The penis and scrotum are adult in size and shape. No further enlargement takes place after stage 5 is reached.
Pubic hair growth

Stage 5
The hair is now like adult pubic hair in both type and quantity. It is distributed in the classic triangle pattern and has spread to the inner thigh area.
Adolescent Medicine Secrets. Philadelphia, PA: Hanley & Belfus; 2002:21-28.
Imaging studies

Left hand/wrist
x-ray to determine bone age9

Cranial MRI
- May identify effects of hypothalamic hamartomas, optic nerve gliomas, hydrocephalus, arachnoidal cysts, and hypothalamic irradiation. These causes can be found in approximately 20% of CPP cases in girls and 65% of cases in boys15

Possible pelvic ultrasound in girls
- May help rule out CPP by identifying ovarian cysts, which may be associated with McCune-Albright syndrome or peripheral precocious (pseudo-) puberty (PPP)1
- Can enable comparison of ovarian and uterine sizes with reference levels. Increased ovarian volume may indicate CPP1,4
Laboratory studies
The healthcare provider may perform ultra-sensitive hormonal assays to confirm the diagnosis of CPP, which include but are not limited to9:
- Testosterone
- Estradiol
- Follicle-stimulating hormone
- Luteinizing hormone
- Thyroid-stimulating hormone
- Thyroxine
- Human chorionic gonadotropin
The pediatric endocrinologist may also perform a GnRH stimulation test.9
TREATMENT

How is CPP treated?
GnRH agonists are standard of care for treatment of CPP16,17
- Since the 1980s, GnRH agonists have been used to suppress the HPG axis1,18
- By desensitizing and downregulating GnRH receptors, GnRH agonists gradually inhibit gonadotropin release1,2,19
GnRH=gonadotropin-releasing hormone; HPG=hypothalamic-pituitary-gonadal.

Learn more about the efficacy of LUPRON DEPOT-PED for the treatment of CPP